

Sperm donation is the provision (or "donation") by a man (known as a sperm donor) of his sperm (known as donor sperm), principally for it to be used in the artificial insemination of a female or females who are not his sexual partners.
Sperm may be donated privately and directly to the intended recipient, or through a sperm bank or fertility clinic. Sperm donation enables a man to father a child for third-party females, and is therefore, categorized as a form of third party reproduction. Pregnancies are usually achieved by using donor sperm in assisted reproductive technology (ART) techniques which include artificial insemination (either by intracervical insemination (ICI) or intrauterine insemination (IUI) in a clinic, or intravaginal insemination at home). Less commonly, donor sperm may be used in in vitro fertilization (IVF).
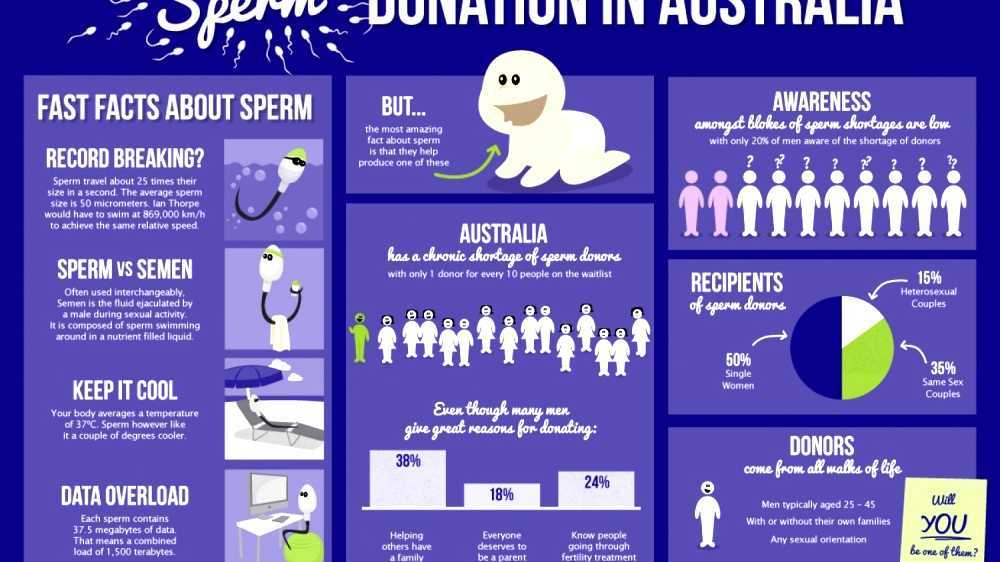
The primary recipients of donor sperm are single women, lesbian couples and heterosexual couples suffering from male infertility.
Donor sperm and 'fertility treatments' using donor sperm may be obtained at a sperm bank or fertility clinic. Here, the recipient may select donor sperm on the basis of the donor's characteristics, such as looks, personality, academic ability, race, and many other factors. Sperm banks or clinics may be subject to state or professional regulations, including restrictions on donor anonymity and the number of offspring that may be produced, and there may be other legal protections of the rights and responsibilities of both recipient and donor. Some sperm banks, either by choice or regulation, limit the amount of information available to potential recipients; a desire to obtain more information on donors is one reason why recipients may choose to use a known donor or private donation.
However conception is achieved, the nature and course of the pregnancy will be the same as one achieved by sexual intercourse, and the male donor will be the biological father of any child born from his donations.
A sperm donor is generally not intended to be the legal or de jure father of a child produced from his sperm. The law may however, make implications in relation to legal fatherhood or the absence of a father. Where sperm is donated by natural insemination,i.e. where the donor has sexual intercourse with the recipient woman, the law in every country will always provide that the male is the father of any child produced, even where the sperm is provided by a third party male who is not the woman's usual sexual partner and where the express intention was to secure a pregnancy.
Video Sperm donation
Laws
Laws regulating sperm donation address issues such as permissible reimbursement or payment to sperm donors, rights and responsibilities of the donor towards his biological offspring, the child's right to know his/her father's identity, and procedural issues. Laws vary greatly from jurisdiction to jurisdiction. In general, laws are more likely to disregard the sperm donor's biological link to the child, so that he will neither have child support obligations nor rights to the child. In the absence of specific legal protection, courts may order a sperm donor to pay child support or recognize his parental rights, and will invariably do so where the insemination is carried out by natural, as opposed to artificial means.
Laws in many jurisdictions limit the number of offspring that a sperm donor can give rise to, and who may be a recipient of donor sperm.
Maps Sperm donation
Uses
Donor sperm is prepared for use in artificial insemination in intrauterine insemination (IUI) or intra-cervical insemination (ICI). Less commonly, donor sperm is prepared for use in other assisted reproductive techniques such as IVF and intracytoplasmic sperm injection (ICSI). Donor sperm may also be used in surrogacy arrangements either by artificially inseminating the surrogate (known as traditional surrogacy) or by implanting in a surrogate embryos which have been created by using donor sperm together with eggs from a donor or from the 'commissioning female' (known as gestational surrogacy). Spare embryos from this process may be donated to other women or surrogates. Donor sperm may also be used for producing embryos with donor eggs which are then donated to a female who is not genetically related to the child she produces.
In medical terms, using donor sperm to achieve a pregnancy is no different from using sperm from a female's male partner.
Procedures of any kind, e.g., artificial insemination or IVF, using donor sperm to impregnate a female who is not the partner of, nor related to the male who provided the sperm, may be referred to as donor treatments.
A Swedish study concluded that 94% of potential donors would be willing to donate to single women and 85% would be willing to donate to lesbian single women or lesbian couples. A review of two studies found that 50 to 68% of actual donors would donate for lesbian couples, and 40 to 64% would donate to single women.

Provision
A sperm donor may donate sperm privately or through a sperm bank, sperm agency, or other brokerage arrangement. Private donors most commonly choose artificial insemination.
Generally, a male who provides sperm as a sperm donor gives up all legal and other rights over the biological children produced from his sperm. However, in private arrangements, some degree of co-parenting may be agreed, although the enforceability of those agreements varies by jurisdiction.
Donors may or may not be paid, according to local laws and agreed arrangements. Even in unpaid arrangements, expenses are often reimbursed. Depending on local law and on private arrangements, men may donate anonymously or agree to provide identifying information to their offspring in the future. Private donations facilitated by an agency often use a "directed" donor, when a male directs that his sperm is to be used by a specific person. Non-anonymous donors are also called "known donors", "open donors" or "identity disclosure donors".
A review of surveys among donors came to the results that the media and advertising are most efficient in attracting donors, and that the internet is becoming increasingly important in this purpose. Recruitment via couples with infertility problems in the social environment of the sperm donor does not seem to be important in recruitment overall.
Sperm banks
A sperm donor will usually donate sperm to a sperm bank under a contract, which typically specifies the period during which the donor will be required to produce sperm, which generally ranges from six to 24 months depending on the number of pregnancies which the sperm bank intends to produce from the donor. If a sperm bank has access to world markets e.g. by direct sales, or sales to clinics outside their own jurisdiction, a male may donate for a longer period than two years, as the risk of consanguinity is reduced (although local laws vary widely).
The contract may also specify the place and hours for donation, a requirement to notify the sperm bank in the case of acquiring a sexual infection, and the requirement not to have intercourse or to masturbate for a period of usually 2-3 days before making a donation.
Sperm provided by a sperm bank will be produced by a donor attending at the sperm bank's premises in order to ascertain the donor's identity on every occasion. The donor masturbates to provide an ejaculate or by the use of an electrical stimulator, although a special condom, known as a collection condom, may be used to collect the semen during sexual intercourse. The ejaculate is collected in a small container, which is usually extended with chemicals in order to provide a number of vials, each of which would be used for separate inseminations. The sperm is frozen and quarantined, usually for a period of six months, and the donor is re-tested prior to the sperm being used for artificial insemination.
Sperm agencies
In some jurisdictions, sperm may be donated through an agency. The agency may recruit donors, usually via the Internet. Donors may undergo the same kind of checks and tests required by a sperm bank, although clinics and agencies are not necessarily subject to the same regulatory regimes. In the case of an agency, the sperm will be supplied to the recipient female fresh rather than frozen.
A female chooses a donor and notifies the agency when she requires donations. The agency notifies the donor who must supply his sperm on the appropriate days nominated by the recipient. The agency will usually provide the sperm donor with a male collection kit usually including a collection condom and a container for shipping the sperm. This is collected and delivered by courier and the female uses the donor's sperm to inseminate herself, typically without medical supervision. This process preserves anonymity and enables a donor to produce sperm in the privacy of his own home. A donor will generally produce samples once or twice during a recipient's fertile period, but a second sample each time may not have the same fecundity of the first sample because it is produced too soon after the first one. Pregnancy rates by this method vary more than those achieved by sperm banks or fertility clinics. Transit times may vary and these have a significant effect on sperm viability so that if a donor is not located near to a recipient female the sperm may deteriorate. However, the use of fresh, as opposed to frozen, semen will mean that a sample has a greater fecundity and can produce higher pregnancy rates.
Sperm agencies may impose limits on the number of pregnancies achieved from each donor, but in practice this is more difficult to achieve than for sperm banks where the whole process may be more regulated. Most sperm donors only donate for a limited period, however, and since sperm supplied by a sperm agency is not processed into a number of different vials, there is a practical limit on the number of pregnancies which are usually produced in this way. A sperm agency will, for the same reason, be less likely than a sperm bank to enable a female to have subsequent children by the same donor.
Sperm agencies are largely unregulated and, because the sperm is not quarantined, may carry sexually transmitted diseases. This lack of regulation has led to authorities in some jurisdictions bringing legal action against sperm agencies. Agencies typically insist on STI testing for donors, but such tests cannot detect recent infections. Donors providing sperm in this way may not be protected by laws which apply to donations through a sperm bank or fertility clinic and will, if traced, be regarded as the legal father of each child produced.
Private or "directed" donations
Couples or individuals who need insemination by a third-party may seek assistance privately and directly from a friend or family member, or may obtain a "private" or "directed" donation by advertising or through a broker. A number of web sites seek to link recipients with sperm donors, while advertisements in gay and lesbian publications are common.
Recipients may already know the donor, or if arranged through a broker, the donor may meet the recipients and become known to them. Some brokers facilitate contact that maintains semi-anonymous identities for legal reasons. Where a private or directed donation is used, sperm need not be frozen.
Private donations may be free of charge - avoiding the significant costs of a more medicalised insemination - and fresh rather than frozen semen is generally deemed to increase the chances of pregnancy. However, they also carry higher risks associated with unscreened sexual or body fluid contact. Legal treatment of donors varies across jurisdictions, and in most jurisdictions (e.g., Sweden) personal and directed donors lack legal safeguards that may be available to anonymous donors. However, the laws of some countries (e.g. New Zealand) recognize written agreements between donors and recipients in a similar way to donations through a sperm bank.
Kits are available, usually on-line, for artificial insemination for private donor use, and these kits generally include a collection pot, a syringe, ovulation tests and pregnancy tests. A vaginal speculum and a soft cup may also be used. STI testing kits are also available but these only produce a 'snap-shot' result and, since sperm will not be frozen and quarantined, there will be risks associated with it.
Natural insemination
Insemination through sexual intercourse is known as natural insemination (NI). Where natural insemination is carried out by a person who is not the woman's usual sexual partner, and in circumstances where the express intention is to secure a pregnancy, this may be referred to as 'sperm donation by natural insemination'. Natural insemination has not been recognised in any state as other than a natural procreation process whereby the sperm donor and biological father is liable for care and support of the child. A woman who becomes pregnant through natural insemination will therefore always have a legal right to claim child support from the donor and the donor has a legal right to the custody of the child. }}</ref> Conceiving through natural insemination is considered a natural process, so the biological father will always be liable for child support and custody rights of the child. The law therefore makes a fine distinction based on the method of conception: the biological relationship between the father and the child and the reason for the pregnancy having been achieved will be the same whether the child was conceived naturally or by artificial means, but the legal position will be different. In some countries and in some situations, sperm donors may be legally liable for any child they produce, but with NI the legal risk of paternity for a donor is always absolute. Natural insemination donors will therefore often donate without revealing their identity.
Despite this,some private sperm donors offer both natural and artificial insemination, or they may offer natural insemination after attempts to achieve conception by artificial insemination have failed. Some women also seek natural insemination for various reasons including the desire by them for a "natural" conception.
Natural insemination by a donor usually avoids the need for costly medical procedures that may require the intervention of third parties. It may lack some of the safety precautions and screenings usually built into the artificial insemination process but proponents claim that it produces higher pregnancy rates. A more 'natural' conception does not involve the intervention and intrusion of third parties. However, it has not been medically proved that natural insemination has an increased chance of pregnancy.
NI is generally only carried out at the female's fertile time, as with other methods of insemination, in order to achieve the best chances of a pregnancy.

Sperm bank processes
A sperm donor is usually advised not to ejaculate for two to three days before providing the sample, to increase sperm count. A sperm donor produces and collects sperm at a sperm bank or clinic by masturbation or during sexual intercourse with the use of a collection condom.
Preparing the sperm
Sperm banks and clinics may "wash" the sperm sample to extract sperm from the rest of the material in the semen. Unwashed semen may only be used for ICI (intra-cervical) inseminations, to avoid cramping, or for IVF/ICSI procedures. It may be washed after thawing for use in IUI procedures. A cryoprotectant semen extender is added if the sperm is to be placed in frozen storage in liquid nitrogen, and the sample is then frozen in a number of vials or straws. One sample will be divided into 1-20 vials or straws depending on the quantity of the ejaculate, whether the sample is washed or unwashed, or whether it is being prepared for IVF use. Following analysis of an individual donor's sperm, straws or vials may be prepared which contain differing amounts of motile sperm post-thaw. The number of sperm in a straw prepared for IVF use, for example, will be significantly less than the number of motile sperm in a straw prepared for ICI or IUI and there will therefore be more IVF straws per ejaculate. Following the necessary quarantine period, the samples are thawed and used to inseminate women through artificial insemination or other ART treatments.
Medical issues
Screening
Sperm banks typically screen potential donors for genetic diseases, chromosomal abnormalities and sexually transmitted infections that may be transmitted through sperm. The screening procedure generally also includes a quarantine period, in which the samples are frozen and stored for at least six months after which the donor will be re-tested for sexually transmitted diseases (STIs). This is to ensure no new infections have been acquired or have developed during the period of donation. Providing the result is negative, the sperm samples can be released from quarantine and used in treatments. Children conceived through sperm donation have a birth defect rate of almost a fifth compared to the general population.
Samples required per donor offspring
The number of donor samples (ejaculates) that is required to help give rise to a child varies substantially from donor to donor, as well as from clinic to clinic. However, the following equations generalize the main factors involved:
For intracervical insemination:
- N is how many children a single sample can help give rise to.
- Vs is the volume of a sample (ejaculate), usually between 1.0 mL and 6.5 mL
- c is the concentration of motile sperm in a sample after freezing and thawing, approximately 5-20 million per ml but varies substantially
- rs is the pregnancy rate per cycle, between 10% to 35%
- nr is the total motile sperm count recommended for vaginal insemination (VI) or intra-cervical insemination (ICI), approximately 20 million pr. ml.
The pregnancy rate increases with increasing number of motile sperm used, but only up to a certain degree, when other factors become limiting instead.
With these numbers, one sample would on average help giving rise to 0.1-0.6 children, that is, it actually takes on average 2-5 samples to make a child.
For intrauterine insemination, a centrifugation fraction (fc) may be added to the equation:
- fc is the fraction of the volume that remains after centrifugation of the sample, which may be about half (0.5) to a third (0.33).
On the other hand, only 5 million motile sperm may be needed per cycle with IUI (nr=5 million)
Thus, only 1-3 samples may be needed for a child if used for IUI.
Using ART treatments such as IVF can result in one donor sample (or ejaculate) producing on average considerably more than one birth. However, the actual number of births per sample will depend on the actual ART method used, the age and medical condition of the female bearing the child, and the quality of the embryos produced by fertilization. Donor sperm is less commonly used for IVF treatments than for artificial insemination. This is because IVF treatments are usually required only when there is a problem with the female conceiving, or where there is a 'male factor problem' involving the female's partner. Donor sperm is also used for IVF in surrogacy arrangements where an embryo may be created in an IVF procedure using donor sperm and this is then implanted in a surrogate. In a case where IVF treatments are employed using donor sperm, surplus embryos may be donated to other women or couples and used in embryo transfer procedures. When donor sperm is used for IVF treatments, there is a risk that large numbers of children will be born from a single donor since a single ejaculate may produce up to 20 straws for IVF use. A single straw can fertilise a number of eggs and these can have a 40% to 50% pregnancy rate. 'Spare' embryos from donor treatments are frequently donated to other women or couples. Many sperm banks therefore limit the amount of semen from each donor which is prepared for IVF use, or they may restrict the period of time for which such a donor donates his sperm to perhaps as little as three months (about nine or ten ejaculates).
Choosing donors
Information about donor
In the US, sperm banks maintain lists or catalogues of donors which provide basic information such as racial origin, skin color, height, weight, color of eyes, and blood group. Some of these catalogues are available via the Internet, while others are only made available to patients when they apply for treatment. Some sperm banks make additional information about each donor available for an additional fee, and others make additional basic information known to children produced from donors when those children reach the age of eighteen. Some clinics offer "exclusive donors" whose sperm is only used to produce pregnancies for one recipient female. How accurate this is, or can be, is not known, and neither is it known whether the information produced by sperm banks, or by the donors themselves, is true. Many sperm banks will, however, carry out checks to verify the information requested, such as checking the identity of the donor and contacting his own doctor to verify medical details. Simply because such information is not verifiable does not imply that it is in any way inaccurate, and a sperm bank will rely upon its reputation which, in turn, will be based upon its success rate and upon the accuracy of the information about its donors which it makes available.
In the UK, most donors are anonymous at the point of donation and recipients can only see non-identifying information about their donor (height, weight, ethnicity, etc.). Donors need to provide identifying information to the clinic and clinics will usually ask the donor's GP to confirm any medical details they have been given. Donors are asked to provide a pen portrait of themselves which is held by the HFEA and can be obtained by the adult conceived from the donation at the age of 16, along with identifying information such as the donor's name and last known address at 18. Known donation is permitted and it is not uncommon for family or friends to donate to a recipient couple.
Qualities that potential recipients typically prefer in donors include the donors being tall, college educated, and with a consistently high sperm count. A review came to the result that 68% of donors had given information to the clinical staff regarding physical characteristics and education but only 16% had provided additional information such as hereditary aptitudes and temperament or character.
Other screening criteria
Sexually active gay men are prohibited or discouraged from donating in some countries, including the US. Sperm banks also screen out some potential donors based on height, baldness, and family medical history.
Number of offspring
Where a donor donates sperm through a sperm bank, the sperm bank will generally undertake a number of checks to ensure that the donor produces sperm of sufficient quantity and quality and that the donor is healthy and will not pass diseases through the use of his sperm. The donor's sperm must also withstand the freezing and thawing process necessary to store and quarantine the sperm. The cost to the sperm bank for such tests is considerable, which normally means that clinics may use the same donor to produce a number of pregnancies in multiple women.
The number of children permitted from a single donor varies by law and practice. These laws are designed to protect the children produced by sperm donation as well as the donor's natural children from consanguinity in later life: they are not intended to protect the donor himself and those donating sperm will be aware that their donations may give rise to numerous pregnancies in different jurisdictions. Such laws, where they exist, vary from jurisdiction to jurisdiction, and a sperm bank may also impose its own limits. The latter will be based on the reports of pregnancies which the sperm bank receives, although this relies upon the accuracy of the returns and the actual number of pregnancies may therefore be somewhat higher. Nevertheless, sperm banks frequently impose a lower limit on geographical numbers than some jurisdictions and may also limit the overall number of pregnancies permitted from a single donor. The limitation on the number of children which a donor's sperm may give rise to is usually expressed in terms of 'families', on the expectation that children within the family are prohibited from sexual relations under incest laws. In effect, the term family means a "woman" and usually includes the donor's partner or ex-partner, so that multiple donations to the same woman are not counted in the limit. The limits usually apply within one jurisdiction, so that donor sperm may be used in other jurisdictions. There is no limit on the number of donations that can be made to the same woman.
There is no limit to the number of offspring which may be produced from private donors.
Despite laws limiting the number of offspring, some donors may produce substantial numbers of children, particularly where they donate through different clinics, where sperm is onsold or is exported to different jurisdictions, and where countries or jurisdictions do not have a central register of donors.
Sperm agencies, in contrast to sperm banks, rarely impose or enforce limits on the number of children which may be produced by a single donor partly because they are not empowered to demand a report of a pregnancy from recipients and are rarely, if ever, able to guarantee that a female may have a subsequent sibling by the donor who was the biological father of her first or earlier children.
Siblings
Where a female wishes to conceive additional children by sperm donation, she will often wish to use the same donor. The advantage of having subsequent children by the same donor is that these will be full biological siblings, having the same biological father and mother. Many sperm banks offer a service of storing sperm for future pregnancies, but few will otherwise guarantee that sperm from the original donor will be available.
Sperm banks rarely impose limits on the numbers of second or subsequent siblings. Even where there are limits on the use of sperm by a particular donor to a defined number of families (as in the UK) the actual number of children produced from each donor will often be far greater.
Donor payment
The majority of donors who donate through a sperm bank receive some form of payment, although this is rarely a significant amount. A review including 29 studies from 9 countries found that the amount of money donors received varied from $10 to EUR70 per donation or sample. The payments vary from the situation in the United Kingdom where donors are only entitled to their expenses, to the situation with some US sperm banks where a donor receives a set fee for each donation plus an additional amount for each vial stored. At one prominent California sperm bank for example, TSBC, donors receive roughly $50 for each donation which has acceptable motility/survival rates both at donation and at a test-thaw a couple of days later. Because of the requirement for the two-day abstinence period before donation, and geographical factors which usually require the donor to travel, it is not a viable way to earn a significant income. Some private donors may seek remuneration although others donate for altruistic reasons. According to the EU Tissue Directive donors in EU may only receive compensation, which is strictly limited to making good the expenses and inconveniences related to the donation. A survey among sperm donors in Cryos International Sperm bank showed that altruistic as well as financial motives were the main factors for becoming a donor. However, when the compensation was increased 100% in 2004 (to DKK 500) it did not significantly affect the numbers of new donor candidates coming in or the frequency of donations from the existing donors. When the compensation was reduced to the previous level (DKK 250) again one year later in 2005 there was no effect either. This led to the assumption that altruism is the main motive and that financial compensation is secondary.
Equipment to collect, freeze and store sperm is available to the public notably through certain US outlets, and some donors process and store their own sperm which they then sell via the Internet.
The selling price of processed and stored sperm is considerably more than the sums received by donors. Treatments with donor sperm are generally expensive and are seldom available free of charge through national health services. Sperm banks often package treatments into e.g. three cycles, and in cases of IVF or other ART treatments, they may reduce the charge if a patient donates any spare embryos which are produced through the treatment. There is often more demand for fertility treatment with donor sperm than there is donor sperm available, and this has the effect of keeping the cost of such treatments reasonably high.
Onselling
There is a market for vials of processed sperm and for various reasons a sperm bank may sell-on stocks of vials which it holds (known as 'onselling'). Onselling enables a sperm bank to maximize the sale and disposal of sperm samples which it has processed. The reasons for onselling may be where part of, or even the main business of, a particular sperm bank is to process and store sperm rather than to use it in fertility treatments, or where a sperm bank is able to collect and store more sperm than it can use within nationally set limits. In the latter case, a sperm bank may sell on sperm from a particular donor for use in another jurisdiction after the number of pregnancies achieved from that donor has reached its national maximum.

Psychological issues
Informing the child
Many donees do not inform the child that they were conceived through sperm donation, or, when non-anonymous donor sperm has been used, they do not tell the child until they are old enough for the clinic to provide contact information about the donor. Some believe that it is a human right for a person to know who their biological mother and father are, and thus it should be illegal to conceal this information in any way and at any time. For donor conceived children who find out after a long period of secrecy, their main grief is usually not the fact that they are not the genetic child of the couple who have raised them, but the fact that the parent or parents have kept information from or lied to them, causing loss of trust.
There are certain circumstances where the child very likely should be told:
- When many relatives know about the insemination, so that the child might find it out from somebody else.
- When the adoptive father carries a significant genetic disease, relieving the child from fear of being a carrier.
The parents' decision-making process of telling the child is influenced by many intrapersonal factors (such as personal confidence), interpersonal factors, as well as social and family life cycle factors. For example, health care staff and support groups have been demonstrated to influence the decision to disclose the procedure. The appropriate age of the child at disclosure is most commonly given at between 7 and 11 years.
Single mothers and lesbian couples are more likely to disclose from a young age. Donor conceived children in heterosexual coupled families are more likely to find out about their disclosure from a third party.
Families sharing same donor
Having contact and meeting among families sharing the same donor generally has positive effects. It gives the child an extended family and helps give the child a sense of identity by answering questions about the donor. It is more common among open identity-families headed by single men/women. Less than 1% of those seeking donor-siblings find it a negative experience, and in such cases it is mostly where the parents have disagreed with each other about how the relationship should proceed.
Other family members
Parents of donors, who are the grandparents of donor offspring and may therefore be the oldest surviving progenitors, may regard the donated genetic contribution as a family asset, and may regard the donor conceived people as their grandchildren.
A review came to the result that a minority of actual donors involved their partner in the decision-making process of becoming a donor. In one study, 25% of donors felt they needed permission from their partner. In another study, however, 37% of donors with a partner did not approve of a consent form for partners and rather felt that donors should make their own decisions. In a Swedish study, donors reported either enthusiastic or neutral responses from their partners concerning sperm donation.
Mother-child relation
Studies have indicated that donor insemination mothers show greater emotional involvement with their child, and they enjoy motherhood more than mothers by natural conception and adoption. Compared to mothers by natural conception, donor insemination mothers tend to show higher levels of disciplinary aggression.
Studies have indicated that donor insemination fathers express more warmth and emotional involvement than fathers by natural conception and adoption, enjoy fatherhood more, and are less involved in disciplining their adolescent. Some donor insemination parents become overly involved with their children.
Adolescents born through sperm donation to lesbian mothers have reported themselves to be academically successful, with active friendship networks, strong family bonds, and overall high ratings of well-being. It is estimated that over 80% of adolescents feel they can confide in their mothers, and almost all regard their mothers to be good role models.
Motivation vs reluctance to donate
A systematic review came to the result that altruism and financial compensation are the main motivations to donate, and to a lesser degree procreation or genetic fatherhood and questions about the donor's own fertility. Financial compensation is generally more prevalent than altruism as a motivation among donors in countries where the compensation is large, which is largely explained by a larger number of economically driven people becoming donors in such countries. Among men who do not donate, the main reason thereof has been stated to be a lack of motivation rather than concerns about the donation.
Reluctance to donate may be caused by a sense of ownership and responsibility for the well-being of the offspring.
Support for donors
In the UK, the National Gamete Donation Trust is a charity which provides information, advice and support for people wishing to become egg, sperm or embryo donors. The Trust runs a national helpline and online discussion list for donors to talk to each other.
In one Danish study, 40% of donors felt happy thinking about possible offspring, but 40% of donors sometimes worried about the future of resulting offspring.
A review came to the result that one in three actual donors would like counselling to address certain implications of their donation, expecting that counselling could help them to give their decision some thought and to look at all the involved parties in the donation.
A systematic review in 2012 came to the conclusion that the psychosocial needs and experiences of the donors, and their follow-up and counselling are largely neglected in studies on sperm donation.

Ethical and legal issues
Anonymity
Anonymous sperm donation occurs under the condition that recipients and offspring will never learn the identity of the donor. A non-anonymous donor, however, will disclose his identity to recipients. A donor who makes a non-anonymous sperm donation is termed a known donor, an open identity donor, or an identity release donor.
Non-anonymous sperm donors are, to a substantially higher degree, driven by altruistic motives for their donations.
Even in the case of anonymous donation, some information about the donor may be released to recipients at the time of treatment. Limited donor information includes height, weight, eye, skin and hair colour. In Sweden, this is the extent of disclosed information. In the US, however, additional information may be given, such as a comprehensive biography and sound/video samples.
Several jurisdictions (e.g., Sweden, Norway, the Netherlands, Britain, Switzerland, Australia and New Zealand, and others) only allow non-anonymous sperm donation. This is generally based on the principle that a child has a right to know his or her biological origins. In 2013, a German court precedent was set based on a case brought by a 21-year-old woman. Generally, these jurisdictions require sperm banks to keep up-to-date records and to release identifying information about the donor to his offspring after they reach a certain age (15-18). See Sperm donation laws by country.
Attitudes towards anonymity
For most sperm recipients, anonymity of the donor is not of major importance at the obtainment or tryer-stage. Anonymous sperm is often less expensive. Another reason that recipients choose anonymous donors is concern about the role that the donor or the child may want the donor to play in the child's life. Sperm recipients may prefer a non-anonymous donor if they anticipate disclosing donor conception to their child and anticipate the child's desire to seek more information about their donor in the future. A Dutch study found that lesbian couples are significantly more likely (98%) to choose non-anonymous donors than heterosexual couples (63%). Of the heterosexual couples that opted for anonymous donation, 83% intended never to inform their child of their conception via sperm donation.
For children conceived by an anonymous donor, the impossibility of contacting a biological father or the inability to find information about him can potentially be psychologically burdensome. One study estimated that approximately 67% of adolescent donor conceived children with an identity-release donor plan to contact him when they turn 18.
Among donors and potential donors
Among donors, a systematic review of 29 studies from nine countries concluded that 20-50% of donors would still be willing to donate even if anonymity could not be guaranteed. Between 40 and 97% of donors agree to release non-identifying information such as physical characteristics and level of education. The proportion of actual donors wishing for contact with their offspring varies between 10 and 88%. Most donors are not open to contact with offspring, although more open attitudes are observed among single and homosexual donors. About half of donors feel that degree of involvement should be decided by the intended parents. Some of the donors prefer contact with offspring in a non-visible way, such as where the child can ask questions but the donor will not reveal his identity. One study recruited donors through the Donor Sibling Registry who wanted contact with offspring or who had already made contact with offspring. It resulted that none of the donors said that there was "no relationship", a third of donors felt it was a special relationship, almost like a very good friend, and a quarter felt it was merely a genetic bond and nothing more. Fifteen percent of actual donors considered offspring to be "their own children". On the whole, donors feel that the first step towards contact should come from offspring rather than parents or the donor himself. Some even say that it is the moral responsibility of the donor not to seek contact with offspring.
The same review indicated that up to 37% of donors reported changes in their attitude towards anonymity before and after donation, with one in four being prepared to be more open about themselves after the donation than before (as a "potential donor"). Among potential donors, 30-46% of potential donors would still be willing to donate even if anonymity could not be guaranteed. Still, more than 75% of these potential donors felt positive towards releasing non-identifying information to offspring, such as physical characteristics and level of education. Single or homosexual men are significantly more inclined to release their identity than married, heterosexual men. Potential donors with children are less inclined to want to meet offspring than potential donors without children (9 versus 30% in the review). Potential donors in a relationship are less inclined to consider contact with offspring than single potential donors (7 versus 28% in the review). From US data, 20% would actively want to know and meet offspring and 40% would not object if the child wished to meet but would not solicit a meeting themselves. From Swedish data, where only non-anonymous donation is permitted in clinics, 87% of potential donors had a positive attitude towards future contact with offspring, although 80% of these potential donors did not feel that the donor had any moral responsibilities for the child later in life. Also from UK data, 80% of potential donors did not feel responsible for whatever happened with their sperm after the donation. With variation between different studies, between 33% and 94% of potential donors want to know at least whether or not the donation resulted in offspring. Some of these potential donors merely wanted to know if a pregnancy had been achieved but did not want to know any specific information about the offspring (e.g. sex, date of birth). Other potential donors felt that knowing the outcome of the donation made the experience more meaningful. In comparison, a German study came to the result that 11% of donors actually asked about the outcome in the clinic where they donated.
An Australian study concluded that potential donors who would still be willing to donate without a guarantee of anonymity were not automatically more open to extended or intimate contact with offspring.
Donor tracking
Even when donors choose to be anonymous, offspring may still find ways to learn more about their biological origins. Registries and DNA databases have been developed for this purpose. Registries that help donor-conceived offspring identify half-siblings from other mothers also help avoid accidental incest in adulthood.
Tracking by registries
Offspring of anonymous donors may often have the ability to obtain their biological father's donor number from the fertility clinic or sperm bank used for their birth. They may then share their number on a registry. By finding shared donor numbers, offspring may find their genetic half-siblings. The donor may also find his number on a registry and choose to make contact with his offspring or otherwise reveal his identity.
Tracking by DNA databases
Even sperm donors who have chosen anonymity and not to contact their offspring through a registry are now increasingly being traced by their children. Improved DNA technology has brought into question the possibility of assuring a donor's anonymity. For example, at least one child found his biological father using his own DNA test and internet research, and was able to identify and contact his anonymous donor.
Fertility tourism and international sperm markets
Different factors motivate individuals to seek sperm from outside their home state. For example, some jurisdictions do not allow unmarried women to receive donor sperm. Jurisdictional regulatory choices as well as cultural factors that discourage sperm donation have also led to international fertility tourism and sperm markets.
Sweden
When Sweden banned anonymous sperm donation in 1980, the number of active sperm donors dropped from approximately 200 to 30. Sweden now has an 18-month waiting list for donor sperm. At least 250 Swedish sperm recipients travel to Denmark annually for insemination. Some of this is also due to the fact that Denmark also allows single women to be inseminated.
United Kingdom
After the United Kingdom ended anonymous sperm donation in 2005, the numbers of sperm donors went up, reversing a three-year decline. However, there is still a shortage, and some doctors have suggested raising the limit of children per donor. Some UK clinics import sperm from Scandinavia.
Despite the shortage, sperm exports from the UK are legal and donors may remain anonymous in this context. In 2009 one Danish clinic secured the approval of the HFEA to import sperm via registered clinics for use in the UK. The sperm must have been processed, stored and quarantined in compliance with UK regulations. The donors have agreed to be identified when the children produced with their sperm reach the age of eighteen. The number of children produced from such donors in the UK will, of course, be subject to HFEA rules (i.e. currently a limit of ten families,) but the donors' sperm may be used worldwide in accordance with the clinic's own limit of one child per 200.000 of population, subject to national or local limits which apply. By 2014 the UK was importing nearly 40% of its sperm requirements, up from 10% in 2005.
Korea
Korean Bioethics Law prohibits selling and buying of sperm between clinics, and each donor may only help giving rise to a child to one single couple. It suffers from a shortage.
Canada
Canada prohibits payment for gamete donation beyond the reimbursement of expenses. Many Canadians import purchased sperm from the United States.
United States
The United States, which permits monetary compensation for sperm donors, has had an increase in sperm donors during the late 2000s recession
Social controversy
The use of sperm donation is most common among single women and lesbians. Some sperm banks and fertility clinics, particularly in the US, Denmark and the UK, have a predominance of women being treated with donor sperm who come within these groups. This produces many ethical issues around the ideals of conventional parenting and has wider issues for society as a whole, including the issues of the role of men as parents, family support for children, and financial support for women with children.
The growth of sperm banks and fertility clinics, the use of sperm agencies and the availability of anonymous donor sperm have served to make sperm donation a more respectable, and therefore a more socially acceptable, procedure. The intervention of doctors and others may be seen as making the whole process a respectable and merely a medical procedure which raises no moral issues, where donor inseminations may be referred to as 'treatments' and donor children as 'resulting from the use of a donor's sperm', or 'born following donation' and subsequent children may be described as 'born using the same donor' rather than as biological children of the same male.
A 2009 study has indicated that both men and women view the use of donor sperm with more skepticism compared with the use of donor eggs, suggesting a unique underlying perception regarding the use of male donor gametes.
As acceptance of sperm donation has generally increased, so has the level of questioning as to whether 'artificial' means of conception are necessary, and some donor children too, have been critical of the procedures which were taken to bring them into the world. Against this background has been the increase in the use of NI as a method of sperm donation. However, while some donors may be willing to offer this as a method of impregnation, it has many critics and it also raises further legal and social challenges.
Some donor children grow up wishing to find out who their fathers were, but others may be wary of embarking on such a search since they fear they may find scores of half-siblings who have been produced from the same sperm donor. Even though local laws or rules may restrict the numbers of offspring from a single donor, there are no worldwide limitations or controls and most sperm banks will onsell and export all their remaining stocks of vials of sperm when local maxima have been attained (see 'onselling' above).
One item of research has suggested that donor children have a greater likelihood of substance abuse, mental illness and criminal behavior when grown. However, its motivation and credibility have been questioned.
Coming forward publicly with problems is difficult for donor-conceived people as these issues are very personal and a public statement may attract criticism. Additionally, it may upset their parents if they speak out. A website called Anonymous Us has been set up where they can post details of their experiences anonymously, on which there are many accounts of problems.

Religious responses
There are a wide range of religious responses to sperm donation, with some religious thinkers entirely in support of the use of donor sperm for pregnancy, some who support its use under certain conditions, and some entirely against.
Catholicism
Catholicism officially opposes both the donation of sperm and the use of donor sperm on the basis that it compromises the sexual unity of the marital relationship and the idea "that the procreation of a human person be brought about as the fruit of the conjugal act specific to the love between spouses."
Judaism
Jewish thinkers hold a broad range of positions on sperm donation. Some Jewish communities are totally against sperm donation from donors that are not the husbands of the recipient, while others have approved the use of donor insemination in some form, while liberal communities accept it entirely.
Protestantism
The Southern Baptist Convention holds that sperm donation from a third party violates the marital bond.

History
In 1884, Professor William Pancoast of Philadelphia's Jefferson Medical College performed an insemination on the wife of a sterile Quaker merchant, which may be the first insemination procedure that resulted in the birth of a child. Instead of taking the sperm from the husband, the professor chloroformed the woman, then let his medical students vote which one of among them was "best looking", with that elected one providing the sperm that was then syringed into her cervix. At the husband's request, his wife was never told how she became pregnant. As a result of this experiment, the merchant's wife gave birth to a son, who became the first known child by donor insemination. The case was not revealed until 1909, when a letter by Addison Davis Hard appeared in the American journal Medical World, highlighting the procedure.
Since then, a few doctors began to perform private donor insemination. Such procedures were regarded as intensely private, if not secret, by the parties involved. Records were usually not maintained so that donors could not be identified for paternity proceedings. Technology permitted the use of fresh sperm only, and it is thought that sperm largely came from the doctors and their male staff, although occasionally they would engage private donors who were able to donate on short notice on a regular basis.
In 1945, Mary Barton and others published an article in the British Medical Journal on sperm donation. Barton, a gynecologist, founded a clinic in London which offered artificial insemination using donor sperm for women whose husbands were infertile. This clinic helped conceive 1,500 babies of which Mary Barton's husband, Bertold Weisner, probably fathered about 600.
The first successful human pregnancy using frozen sperm was in 1953.
Donor insemination remained virtually unknown to the public until 1954. In that year the first comprehensive account of the process was published in The British Medical Journal.
Donor insemination provoked heated public debate. In the United Kingdom, the Archbishop of Canterbury established the first in a long procession of commissions that, over the years, inquired into the practice. It was at first condemned by the Lambeth Conference, which recommended that it be made a criminal offence. A Parliamentary Commission agreed. In Italy, the Pope declared donor insemination a sin, and proposed that anyone using the procedure be sent to prison.
Sperm donation gained popularity in the 1980s and 1990s.
In many western countries, sperm donation is now a largely accepted procedure. In the US and elsewhere, there are a large number of sperm banks. A sperm bank in the US pioneered the use of on-line search catalogues for donor sperm, and these facilities are now widely available on the websites of sperm banks and fertility clinics.
Recent years have also seen sperm donation become relatively less popular among heterosexual couples, who now have access to more sophisticated fertility treatments, and more popular among single women and lesbian couples - whose access to the procedure is relatively new and still prohibited in some jurisdictions.
United States
In 1954, the Superior Court of Cook County, Illinois granted a husband a divorce because, regardless of the husband's consent, the woman's donor insemination constituted adultery, and that donor insemination was "contrary to public policy and good morals, and considered adultery on the mother's part." The ruling went on to say that, "A child so conceived, was born out of wedlock and therefore illegitimate. As such, it is the child of the mother, and the father has no rights or interest in said child."
However, the following year, Georgia became the first state to pass a statute legitimizing children conceived by donor insemination, on the condition that both the husband and wife consented in advance in writing to the procedure.
In 1973, the Commissioners on Uniform State Laws, and a year later, the American Bar Association, approved the Uniform Parentage Act. This act provides that if a wife is artificially inseminated with donor semen under a physician's supervision, and with her husband's consent, the husband is legally considered the natural father of the donor inseminated child. That law was followed by similar legislation in many states.
The first commercial sperm bank in the United States opened in Roseville, Minnesota in 1971.
United Kingdom
In the United Kingdom, the Warnock Committee was formed in July 1982 to consider issues of sperm donation and assisted reproduction techniques. Donor insemination was already available in the UK through unregulated clinics such as BPAS. Many of these clinics had started to offer sperm donation before the widespread use of freezing techniques. 'Fresh sperm' was donated to order by donors at the fertile times of patients requiring treatments. Commonly, infertility of a male partner or sterilisation was a reason for treatment. Donations were anonymous and unregulated.
The Warnock Committee's report was published on July 18, 1984. and led to the passing of the Human Fertilisation and Embryology Act 1990. That act provided for a system of licensing for fertility clinics and procedures. It also provided that, where a male donates sperm at a licensed clinic in the UK and his sperm is used at a UK clinic to impregnate a female, the male is not legally responsible for the resulting child.
The 1990 Act also established a UK central register of donors and donor births to be maintained by the Human Fertilisation and Embryology Authority (the 'HFEA'), a supervisory body established by the Act. Following the Act, for any act of sperm donation through a licensed UK clinic that results in a living child, information on the child and the donor must be recorded on the register. This measure was intended to reduce the risk of consanguinity as well as to enforce the limit on the number of births permitted by each donor. The natural child of any donor has access to non-identifying information about their donor, starting at the child's eighteenth birthday.
The emphasis of the 1990 Act was on protecting the unborn child. However, a general shortage of donor sperm at the end of the 20th century, exacerbated by the announcement of the removal of anonymity in the UK, led to concerns about the excessive use of the sperm of some donors. These concerns centered on the export and exchange of donor sperm with overseas clinics, and also the interpretation of the term 'sibling use' to include donated embryos produced from one sperm donor, and successive births by surrogates using eggs from different women but sperm from the same sperm donor. Donors were informed that up to ten births could be produced from their sperm, but the words 'other than in exceptional circumstances' in the consent form could potentially lead to many more pregnancies. These concerns led to the SEED Report commissioned by the HFEA, which was in turn followed by new legislation and rules meant to protect the interests of donors: When a male donates his sperm through a UK clinic, that sperm is not permitted to give rise to more than ten families total, anywhere in the world.

International comparison
On the global market, Denmark has a well-developed system of sperm export. This success mainly comes from the reputation of Danish sperm donors for being of high quality and, in contrast with the law in the other Nordic countries, gives donors the choice of being either anonymous or non-anonymous to the receiving couple. Furthermore, Nordic sperm donors tend to be tall, with rarer features like blond hair or different color eyes and a light complexion, and highly educated and have altruistic motives for their donations, partly due to the relatively low monetary compensation in Nordic countries. More than 50 countries worldwide are importers of Danish sperm, including Paraguay, Canada, Kenya, and Hong Kong. Several UK clinics also export donor sperm, but they must take steps to ensure that the maximum number of ten families produced from each donor is not exceeded. The use of the sperm outside the UK will also be subject to local rules. Within the EU there are now regulations governing the transfer of human tissue including sperm between member states to ensure that these take place between registered sperm banks. However, the Food and Drug Administration (FDA) of the US has banned import of any sperm, motivated by a risk of mad cow disease, although such a risk is insignificant, since artificial insemination is very different from the route of transmission of mad cow disease. The prevalence of mad cow disease is one in a million, probably less for donors. If prevalence was the case, the infectious proteins would then have to cross the blood-testis barrier to make transmission possible. Transmission of the disease by an insemination is approximately equal to the risk of getting killed by lightning.

Fictional representation
Movie plots involving artificial insemination by donor are seen in Made in America, Road Trip, The Back-Up Plan, The Kids Are All Right, The Switch, Starbuck, and Baby Mama, the latter also involving surrogacy.
Films and other fiction depicting emotional struggles of assisted reproductive technology have had an upswing first in the latter part of the 2000s (decade), although the techniques have been available for decades. Yet, the number of people that can relate to it by personal experience in one way or another is ever growing, and the variety of trials and struggles is huge.
A 2012 Bollywood comedy movie, Vicky Donor, was based on sperm donation. The film release saw an effect; the number of men donating sperm increased in India.
A 2017 Kollywood movie Kutram 23 is also a movie based on sperm donation.

See also

References

External links
- Sperm donation in the UK (the UK's regulatory body - lists all UK clinics offering sperm donation)
- Sperm Donation at Curlie (based on DMOZ)
Source of the article : Wikipedia
